
SAN DIEGO — Dr. David Feifel’s vacation in Israel was wrapping up last October when the psychiatrist turned on his cellphone. He scrolled through messages he’d missed during the Jewish holiday but stopped on one text, dumbfounded, and read it over and again.
This isn’t real, he thought, then cried out in despair in front of his wife and children.
One of his patients, a Navy and Marine Corps veteran who for years had battled PTSD, anxiety and depression at his Kadima Neuropsychiatry Institute in La Jolla, had taken her life. In her farewell email, she cited what had, in part, prompted her decision:
The VA San Diego Healthcare System was going to stop covering her ketamine treatments.
Though ketamine has been used for more than 50 years as an anaesthetic — and recreational drug — it has recently shown promise in derailing suicidal thoughts among patients resistant to other treatments. The San Diego VA has referred at least 32 high-risk veterans to Feifel, a recognized expert in the use of ketamine for mental illness, since he opened Kadima in 2017.
But following President Donald Trump’s hype last year over Spravato, a derivative of ketamine he called “incredible” in combating veteran suicides, the San Diego VA began pulling veterans from Kadima to treat them in-house with the controversial nasal spray.
Some of the vets had heard about Spravato but were nevertheless stunned when the VA cut off their ketamine at Kadima without giving advance notice to them, their psychiatrists at the VA or Feifel. In some cases, vets were told less than 24 hours before a scheduled appointment that the treatment they’d relied on for years would no longer be an option.


“I was basically told that it was either their way or the highway,” said AJ Williams, an Army veteran who said she was sexually assaulted during her 14 months in service and developed anxiety and major depression as a result. “I was not consulted. I was not asked if I wanted to do this. I was not given a choice.”
A San Diego VA spokeswoman told inewsource on May 21 that the agency “has communicated to patients and Kadima leaders” that this is happening because the VA is now offering Spravato and intravenous ketamine at its La Jolla Medical Center.


That is not true, said Williams and eight other veterans, along with Feifel and his staff. Eight months of emails between Kadima and the VA also don’t support the spokesperson’s statement. They show a VA psychiatrist reassuring one of his patients that the agency had no intention of taking veterans off ketamine — two weeks before the VA began to do just that.
The veterans also said the VA hasn’t offered them IV ketamine. Unlike Spravato, IV ketamine is very similar to the intramuscular injections given at Kadima in strength, amount absorbed by the body and psychological effect.
“It's just unconscionable that the VA would take the action that they have,” said Dwight Stirling, founder and CEO of the Center for Law and Military Policy, a nonprofit think tank in Huntington Beach. Stirling is also a reserve judge advocate general officer in the California National Guard and a law professor at the University of Southern California.
“The thought of taking patients off of a treatment without first consulting with their doctors is simply indefensible,” he said.


Feifel and his team have spent months trying to fix a situation they believe is dangerous and irresponsible on the part of the VA. Emails he shared with inewsource show VA administrators made assurances, then reneged, or scheduled meetings to clear things up and then canceled.
VA psychiatrists told him they had no idea why the agency was doing this and that they hadn’t been consulted. The vets who had been receiving the treatments said the psychiatrists told them the same thing.


When fear over losing ketamine spread throughout Kadima’s patients, one veteran took her life, and the VA moved quickly to renew a contract that would in theory allow vets to continue treatments at the private clinic. But shortly after, the VA again began to ignore requests from Kadima to renew authorizations for vets to continue treatment — and now Feifel worries history is repeating itself.
He wrote to VA leadership in April: “We were under the impression that the VA learned from its mistake and under no circumstance would it follow the same catastrophic path that resulted in that tragic outcome.
“And yet, here we are, watching a train wreck in slow motion … AGAIN!”
How Ketamine Came To San Diego
The Kadima Neuropsychiatry Institute sits in an unremarkable office building across the street from the San Diego VA and UC San Diego School of Medicine, where Feifel completed his residency in psychiatry in 1995.


Over the following decades, the doctor became increasingly frustrated with his field. He felt the treatments at the time were inadequate for a large portion of the growing population of mentally ill patients, and he worried he’d see no breakthroughs during his career.
But new treatments did emerge. Some he advocated for bringing into UCSD.
The first was transcranial magnetic stimulation, or TMS — a noninvasive therapy that targets regions of the brain with electromagnetism and is now FDA approved for use on depression, OCD and migraines. Feifel, now on the national Clinical TMS Society board of directors, developed the first clinical TMS program at the university.
Then, Feifel said, “ketamine came out of left field.”
The drug was first synthesized in 1962, approved for human use eight years later as an anaesthetic and used on the battlefield during Vietnam. But it wasn’t until the early 2000s that researchers identified ketamine’s potential, at lower doses, to help those with treatment-resistant depression.
Feifel read those early studies and thought: Either the researchers got lucky, or “this is really one of the biggest breakthroughs ever,” he said.
He persuaded UCSD to begin offering ketamine to patients with severe treatment resistant depression, most of whom had suicidal thoughts. It was a slog trying to talk a bureaucracy that large into letting him use a drug off label that has a high potential for abuse.
“It just made it more difficult to convince people that this was not a harebrained idea,” Feifel said. Eventually he got his way and established for the first time a UCSD practice where the drug was administered outside of a research setting for depression and suicidality. The results were impressive.
“This was really something like I've never seen in my years in the field of psychiatry,” Feifel said. “It had limitations, for sure, but it also had characteristics that we had not seen in terms of the ability to improve people's major depression when nothing else did. And also, many times, to do it very, very rapidly.”
His San Diego VA colleagues began sending him high-risk veterans. After recognizing the progress made by patients who had failed with every other treatment, they sent more.


Then a council within the American Psychiatric Association published a consensus statement in 2017 on the use of ketamine to treat mood disorders. A panel of experts had concluded after reviewing existing data from seven clinical trials that there was “compelling evidence that the antidepressant effects of ketamine infusion are both rapid and robust, albeit transient.”
Who’s getting ketamine?
It’s unclear how many VAs are referring patients outside the hospital system for ketamine. A 2017 VA guidance document contains a reference to a survey from fiscal 2015 that found eight VA sites around the country were providing the drug in house for treatment-resistant depression and 22 were providing it offsite. inewsource contacted seven VA hospitals for updated numbers but all refused to provide them by phone or email. Instead, they told reporters to ask for that data through a Freedom of Information Act request, which can take the VA months or even years to fulfill.
Feifel resigned that same year as a UCSD professor emeritus and founder and director of the Psychiatry Department’s advanced treatment program to start Kadima Neuropsychiatry Institute, and the VA continued to refer veterans for both TMS and ketamine treatments.
“By no means does ketamine work for everybody,” Feifel said, but it worked enough for the VA referrals to keep coming.
“One thing about the vets ... they will commonly put it very blankly that, ‘I wouldn't be here were it not for ketamine,’ or ‘Ketamine is what keeps me alive,’” Feifel told inewsource.
And that’s why any “grumblings of a concern” about ketamine being taken away from them “would always create a lot of panic with the patients,” he said.
Euphoria And Horror
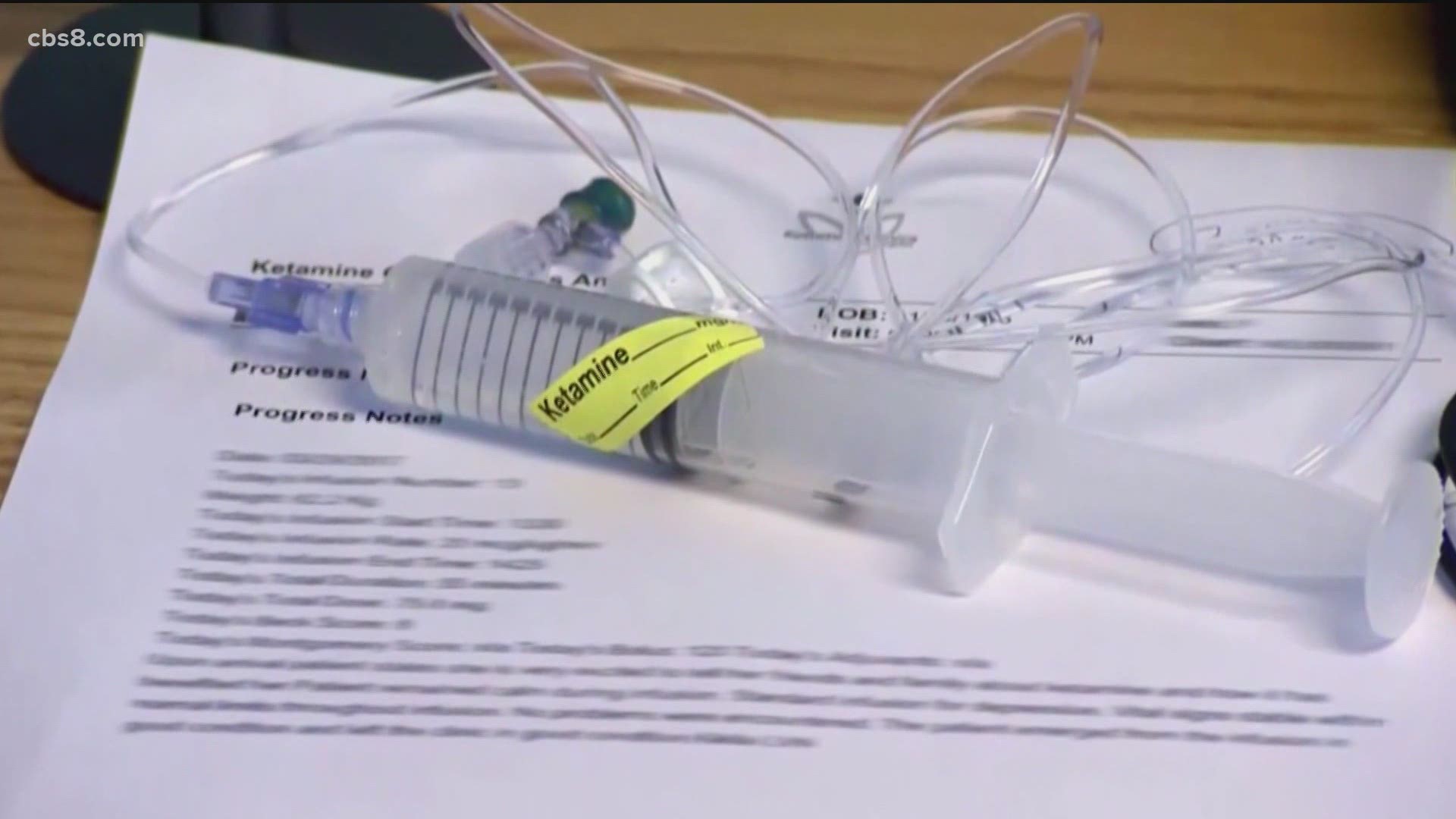
Ketamine infusions at Kadima work like this:
A patient answers a questionnaire about their mental state and health. Feifel then goes over the results with them in a private treatment room furnished with a leather recliner, adjustable colored lighting, noise-canceling headphones and nature-oriented art on the walls.


If the patient is anxious or otherwise high-strung, Feifel may try to comfort them or give them medication like Xanax so the anxiety doesn’t carry over into what comes next. A strap is put around the patient’s wrist for monitoring blood pressure and other vital signs. Then, Feifel determines the proper dosage of ketamine using criteria that can include a patient’s body mass, previous treatment outcomes and current mental state.
The drug is delivered through an injection in the shoulder and a second dose may be given as the effects of the first begin to wane. Within minutes of the first injection, patients typically enter into a psychedelic state that can last for an hour or more. They are carefully monitored by nurses sitting just outside the rooms through a system of closed-circuit cameras.


After patients come out of the psychedelic state, they relay their experience to Feifel, who works with the patient to process the experience’s positive effect into their daily life.
In mid-May, one of those cameras displayed 51-year-old Navy veteran Larry McMinn, who depends on ketamine to keep his barrage of suicidal thoughts at bay. McMinn allowed inewsource to monitor his treatment that day from beginning to end.
Prepared with an audio playlist and headphones, McMinn settled into the recliner after the first injection. Roughly an hour later, the veteran emerged slowly from his treatment, appearing to be caught halfway between drunk and dreaming.
“You are a godsend,” he told Feifel.
Ketamine’s immediate effects on the mind and body can last several hours, but its impact on eliminating suicidal urges can last patients days, weeks or months.
The trips themselves can range from euphoria to horror.
As was the case with McMinn’s treatment, some are pure bliss. Feifel said he has one patient who often screams out in ecstasy — which makes it awkward when the doctor is consulting with new clients in his office next door.
“I always joke with the nurses that it’s like that scene in ‘When Harry Met Sally,’” Feifel said. “It's like, ‘I'll take what she's getting.’”
Other times, veterans may find themselves back in a war zone, reliving traumatic experiences and screaming out in terror. They can become violent. A loved one may accompany the patients to try to bring them back to earth, hold their hand or otherwise comfort them.
Or a trip can be just plain strange, like when Renee St.Clair thought her brain left her head and she had to be calmed down by Feifel and staff. She still has that treatment session recorded on her phone. It makes her laugh. St.Clair is not a veteran but a former Kadima patient who suffers from major depression. Because most insurance companies won’t cover ketamine treatments, the therapy isn’t really an option for many of the millions living with depression in the U.S. A single treatment at Kadima costs around $400, and a patient typically goes through six to eight sessions just to see if it’s effective.
But St.Clair was lucky. She had the means to pay for it and was one of those for whom the drug worked wonders.


She remembers the moment it did.
“I was in my bed at three in the morning,” St.Clair said. “I had a treatment earlier in the day and I woke up and I saw the moon through my shutters, and it was brighter than it usually is. And I heard crickets outside and they were louder than they usually are. And I was thinking clearer. And I'm like, ‘Oh, my God, this is what it feels like to have that depression gone.’”
That morning she drove to work, where for 11 years she would look out the window of her downtown San Diego law office at the Coronado bridge and think, “One of these days I’m going to jump off that bridge.”
But, she said, “That morning, I got there and I thought, ‘Not today.’”
St.Clair left her career as an attorney to become Kadima’s chief operating officer last July.
But even before then, as a patient at Kadima, she said one person tugged at her heart more than any other: Jodi Maroney, a veteran of the Iraq and Afghanistan wars whose suicide would prompt Feifel and St.Clair to go on record with inewsource about the role they believe the VA played in her death.
A Cautious Optimism
Maroney was a uniquely impressive individual.
She began flying in high school and joined the U.S. Marine Corps her junior year of college. She had three combat deployments between 2002 to 2005, and was one of the first pilots — in a Sikorsky CH-53E Super Stallion — to cross the Iraqi border during Operation Iraqi Freedom.
Maroney transported Marines while under fire in Afghanistan, where she endured repeated rocket attacks at her forward operating base, her husband Jon Maroney told inewsource.
In 2006, she transitioned into the reserves, but continued to spend her time in the air — flying for U.S. Customs and Border Protection.
In her free time, she tutored refugee children at San Diego Refugee Tutoring, volunteered at the Naval Medical Center San Diego’s Surf Clinic for wounded service members, and coached children’s basketball at her vacation bible school’s sports camp.
“We care about all our patients, but it's just natural that there are some people who stand out in certain ways,” Feifel told inewsource.
“And Jodi, I think universally, was one of those patients.”
The stress and trauma of Maroney’s combat experience manifested years after she left Iraq and Afghanistan. It first presented around 2010 as insomnia with
increasing nightmares — a dangerous problem to have when her job involved flying helicopters at night over the ocean. Years later her doctor formally diagnosed her with PTSD.
Her husband told inewsource Maroney tried more than 70 different medications, TMS and, as a last ditch effort, electroconvulsive therapy. Nothing worked. As a result, Maroney began to lose hope that anything would help her symptoms. That led to severe depression and eventually, repetitive thoughts of suicide.
Ketamine, under Feifel’s supervision, was about the only thing that would take away those suicidal impulses, he said.
On good days, the treatment could bring a smile to Maroney’s face that her husband still can’t discuss without falling apart. Other times, it would have no effect.

“The thing that I hate about ketamine is you can’t bank on it,” Maroney’s husband told inewsource.
“You can't go in there and say, ‘Hey, things are really bad. OK, let's break glass. Let's get ketamine and you're going to be right as rain.’”
Though the response rate hovers a little above 50%, there is no reliable way of predicting who will respond well to ketamine, said Dr. Robert Meisner, medical director of the ketamine service program at McLean Hospital in Massachusetts.
“It is critical that patients know before considering any psychiatric intervention for severe depression that there very rarely is a magic bullet,” Meisner said.
But with ketamine, he said, “If ever in the past several decades there has been reason for cautious optimism regarding new developments for the treatment of depression and some other disorders, now appears to be one of those moments.”
That optimism is sorely needed.
As Meisner pointed out, suicide is the second leading cause of death in the U.S. for people ages 10 to 34. Major depressive disorder is the leading cause of disability worldwide. And one person takes their life every 40 seconds.
“If we were talking about a disease associated with just about any other organ system, this would be front page news over and over again,” he said. “And yet somehow, in the cultural discourse of contemporary America, we've turned our head away from what is a daily tragedy.”
Among veterans, the suicide rate for those 18 to 34 years old increased by 76% from 2005 to 2017. An average of about 17 veterans took their life each day in 2017.
“That is astounding to me,” Meisner said.
Suicide Prevention Help - If you are having thoughts of suicide, you can call the National Suicide Prevention Lifeline at (800) 273-8255 or the San Diego Access and Crisis Line at (888) 724-7240. Other resources are available here.
Those numbers have prompted the Trump administration to try something new — a nasal spray derivative of ketamine manufactured by Johnson & Johnson called Spravato, which was fast-tracked through the FDA approval process in March 2019.
“It really takes that horrible anxiety, whatever causes somebody to be so desperate to commit suicide, you take it, it's an inhaler, and you take it and its results are incredible,” Trump told an AMVETS convention last August.
“And I’ve instructed the top officials to go out and get as much of it as you can,” the president said.
But as happened this year with hydroxychloroquine and COVID-19, Trump’s promotion for Spravato came without solid research supporting his claims, which became a problem nationally and in San Diego.
Spravato And Its Effectiveness
Researchers, medical experts and VA doctors questioned Spravato’s effectiveness and safety following Trump’s public remarks about the drug last year.
The VA’s Medical Advisory Panel voted against including the nasal spray in the agency’s formulary — a list of drugs and supplies that must be available for prescription at all VA facilities — but still approved its use on a limited basis which requires veterans try other treatment options first.
In June 2019, the chairman of the House Committee on Veterans’ Affairs, Democratic Rep. Mark Takano of Riverside, called for more information about the VA’s review and contracting process for Spravato.
Takano did so following an investigation by the nonprofit Center for Public Integrity about the influencing factors behind the drug’s rapid adoption. The investigation found the pharmaceutical company behind Spravato was working with Trump associates from his Mar-a-Lago Club and that the president had offered to help the VA negotiate purchases of the drug from the manufacturer, Johnson & Johnson.
The investigation did not uncover how Trump learned about Spravato or the extent of his influence on the VA’s decisions. Neither the White House, the VA nor the Mar-a-Lago associates would talk to the reporter on the story.
“Questions remain about the ultimate impact on the health and safety of veterans, who should not be made into a ‘test case’ while the clinical community continues to gather data about this treatment,” Takano said.
Locally, a spokesperson for Rep. Scott Peters, D-San Diego, told inewsource the congressman’s office is aware of the House committee’s investigation and is urging any San Diego veterans being transitioned to Spravato against their wishes to contact him.
How To Contact Your Representative - If you are unsure who represents you in Congress, use this online tool to search by your ZIP code. It will list your representatives and provide contact information.
“Serving our veterans is a top priority for Rep. Peters and a big part of what we do at our San Diego office is advocate for veterans who don’t feel they are getting the quality care they deserve from the VA,” said Peters’ chief of staff, MaryAnne Pintar.
Meisner, the ketamine expert from McLean hospital, said he’s seen both Spravato and IV ketamine work well for patients, and that “one cannot say in a categorical way” whether either drug is superior to the other.
“I do not think we have enough data or experience,” he said.
Ten of the country’s 170 VA medical centers are administering Spravato, and 43 veterans have received the drug as of May 13, a VA spokesperson said.


The VA San Diego Healthcare System is one of those 10, and Joel Andrews is one of the veterans receiving it.
Andrews, who served in the Army and spent his last few years as part of the Old Guard at Arlington National Cemetery, spoke with inewsource at Kadima on May 15, a few hours after receiving his second Spravato treatment.


“It didn't really do anything,” he said.
Andrews received ketamine treatments at Kadima for two years before a VA psychiatrist notified him in early May that he was cut off. When he asked why, he said he got no definitive answer. He emailed leadership at the San Diego VA, including the director, associate director and medical director, but said he received no response. He sent a letter to the U.S. Senate Committee on Veterans’ Affairs:
“I have been getting IV ketamine for approximately two years now, it has helped me tremendously. I receive treatment on a weekly basis. I believe this lesser treatment will not be beneficial for the vets already going to Kadima. I am really frustrated with the VA and the way in which they treat the mental health patients like pawns.”


Staff at the committee thanked him for his letter and said they sent it up the chain.
“It's frustrating because nobody has a definitive answer as to what the hell is going on with all of this,” Andrews said. “It's like they're playing some game and they're trying to keep it a secret.”


It’s a dangerous game. When Feifel first learned of the San Diego VA’s actions in late September, the doctor thought that even mentioning the problem to his patients could trigger a terrible response. Working with their loved ones, Feifel
tried to keep the news from some who hadn’t yet been alerted by the VA — then paid for their treatments himself while scrambling to find a solution.
It didn’t work.
Jodi’s Legacy
On Sept. 30, the VA called Kadima and told the receptionist to stop treating veterans by the end of the day.
“They didn’t ask to talk to Dr. Feifel. They didn’t ask to speak to management,” said St.Clair. “They told the receptionist.”
She immediately called Feifel, and the two agreed they would continue to treat the approximately 20 patients scheduled that week — against the VA’s directive.
“If they showed up and we said, ‘No, the VA said you're not authorized. Go home,’ it would have been absolutely disastrous,” St.Clair told inewsource.
“It wasn't medically correct. It wasn't ethically correct. It wasn't humanistically correct,” she said, adding that the VA “missed it on every single box.”
St.Clair was told by VA staff that the “status of any future authorized care” for vets at Kadima is “currently pending,” and there was no “exact timeline on when this will be approved.” She emailed back, warning there were “serious and significant factors at play if Kadima follows the VA’s advisement and cuts off vet patient care.”


On Oct. 1, the VA had no new information for Kadima about how the clinic should proceed with the veterans under its care. On Oct. 2, Feifel forwarded a veteran testimonial to VA officials which said that ketamine treatment at Kadima
“prevents me from killing myself for a solid week or two.” The following day, he forwarded that email to San Diego VA Director Robert Smith.
On Oct. 4, San Diego VA Chief of Staff and Medical Director Dr. Kathleen Kim responded. “We sincerely apologize for the gap in services,” Kim wrote, and explained the snafu was due to the Mission Act, a law that expanded healthcare offerings to veterans.
Yet despite calling for a cutoff in treatment, the VA wasn’t offering an alternative for the veterans at Kadima. At that time, the agency wasn’t providing Spravato in house.
Feifel again forwarded along messages he was receiving from distraught patients to the VA:
“The VA just cut it off so they’re leaving a whole bunch of people stranded … like myself, who have suicidal ideation and they’re going to pull the trigger,” one said.
A second patient wrote to Feifel that “it does not sit well with me” that the VA would “stop a treatment that is producing positive results without explanation or concern or a hint of when a decision will be made.”
Another had a panic attack during a ketamine treatment, Feifel said, which the doctor attributed to the patient’s anger and worry about his potential future at Kadima.
VA officials responded and asked Feifel to continue treating veterans while they fast-tracked an administrative process to get things fixed. Feifel agreed.
On Oct. 7, Jon Maroney texted Feifel to let him know his wife had heard from VA psychiatrists about “the potential of losing ketamine.” Feifel urged him to contact the VA, which he did.
“I called the Director’s Office and spoke to the Chief of Staff. I told them how big of an impact this would be. I only hope it helps. She is devastated right now,” Maroney’s husband told Feifel that day.
Still nothing happened. Then, on Oct. 14 — two weeks into Kadima’s struggle with the VA — Maroney took her life.
The next day, the VA chief of psychiatry emailed Kadima that he was “happy to report” that he’d submitted the proper paperwork to get things sorted out.
Three days later, all veterans were good to go for ketamine treatment, Maroney being one of them.
“Congratulations, Jodi,” said St.Clair sarcastically.
Calm, restrained and optimistic, Feifel reassured St.Clair that the VA would learn its lesson from this. The renewed agreement between the agency and Kadima would be Jodi’s legacy, he said.


“Like, we lost one but saved the rest,” St.Clair remembered.
At the time, Feifel thought it an ironic coincidence that the agreement happened so quickly after Maroney’s death — had she hung in a bit longer, everything would have been back to normal.
But he soon discovered that VA leadership had heard of the suicide, which is why, he believes, they moved so fast after weeks of inaction.
“I figured if there's a silver lining to this horrible, horrible tragedy, it’s that the VA now understands what's at stake here, and hopefully things will get the attention they need,” Feifel told inewsource.
But that’s not what happened.
Recurring dreams
Even with the new agreement in place, emails show St.Clair spent January, February and early March trying to obtain authorizations for veterans. She was passed off from one department to the next, and left voicemails and emails that went unreturned. On March 11, Feifel emailed top San Diego VA administrators requesting a meeting.
“Like last October, we find ourselves in a situation in which we are continuing to treat veterans without VA authorizations and without reimbursement in order not to disrupt their access to this treatment,” he wrote. “Like last October, the veterans we treat are receiving letters that their care is being denied, which once again is causing confusion, upset and/or anger.”
VA officials eventually responded, set up a time for a meeting, canceled that meeting, then never rescheduled.
On April 7, Feifel emailed top administrators again with the subject line, “WILL IT REQUIRE ANOTHER VETERAN TO COMMIT SUICIDE?” The doctor attached more than 30 pages documenting the VA’s unresponsiveness over the past seven months and wrote that it exemplified the VA’s “ludicrously broken system.”
In the body of his email, Feifel gave up all semblance of civility.
“I find it remarkable that I have written an email as blunt and openly angry as this one. Me and my team have acted with great restraint in our dealings with the VA even after Jodi’s suicide, which upset us very much especially because it was
clearly preventable. But we are finding it increasingly difficult to be patient with the non-responsiveness and incompetence which we feel is utterly inexcusable.”
Some Kadima vets emailed Dr. Susan Trompeter, the San Diego VA Community Care medical director, or spoke with their primary care psychiatrist at the VA, Dr. David Printz, to express their dismay over the VA’s actions.
Trompeter responded by email to at least two veterans in March that the VA was “evaluating all requests for additional ketamine treatment(s) from Kadima.” Printz, the psychiatrist for many of the veterans interviewed for this story, reassured one of them in an April 17 email that “the VA has no intention of discontinuing ketamine treatment in the community.”
Two weeks after that reassurance, Printz let Kadima know that the VA would be pulling veterans from the clinic and transitioning them to Spravato. He did not respond to inewsource’s emails or phone calls for an interview.
One of Printz’s patients, Navy veteran McMinn, told inewsource he still has treatments remaining at Kadima under the VA’s authorization but knows that once he runs the course it’s over.
“I gave nine years, five months and 28 days to the United States Navy. I signed a blank check for my life to defend my country,” McMinn said on May 15. The veteran choked up.
“Now that I need them, they're not there for me, and it's not right,” he said.
“You're supposed to take care of me.”


On May 18, inewsource emailed San Diego VA spokesperson Cindy Butler requesting an interview with any or all of the five members of the VA leadership team involved with, or responsible for, the situation at Kadima.
None responded.
Instead, the VA spokesperson provided inewsource with a statement that includes comments that this article has proven to be untrue. The statement said that since January, the VA has established the capacity to provide IV ketamine and Spravato “on-site and has begun transitioning Veterans receiving the treatment back to VA care for better integration with the other VA services they already receive. This is being done in a phased manner and providers have discussed this decision with their patients who receive this type of care.”
As of Monday, 10 veterans have been taken off ketamine at Kadima, with more expected to transition back to the VA once they finish their current course of treatment.
One of them wrote to Feifel on April 28, praising the doctor for his years of treatment, but apologizing in advance.
He would no longer be coming to the clinic, he said, because the VA wasn’t authorizing his treatments and he couldn’t in good conscience let Feifel continue to front the cost.
“You have been a great doctor for me and a real blessing. I know without your treatments I would have ended things for myself. For I had lost all HOPE,” he said.
The veteran wrote that he tried Spravato at the VA, which “might have worked for two hours,” but left him in a worse condition than if he had never taken it.
“I keep having recurring dreams that I take a glock, contact all the news media and stand in the entrance of the VA … and end my life,” he wrote.
“Remember,” he assured Feifel, “it’s just recurring dreams.”
inewsource photo and video journalist Zoë Meyers and intern Natallie Rocha contributed to this report.